Every hospital has a different format and every department has its own template. The result is that critical patient information gets missed, misread, or buried.
Medical reports serve more than one purpose. They are clinical documents, legal records, and communication tools between care teams. When the format is inconsistent, information that one doctor considers essential may not even appear in the version the next doctor receives. This creates medical as well as legal risks.
In this article, I will walk you through a standard medical report format that works across specialties and care settings. I reviewed 15+ sample medical reports across specialties to put this guide together.
Medical report format structure
According to data from PubMed, documentation errors account for 23% of all hospital errors, making them one of the most common error types, above medication errors and technical failures. A missing allergy note, an undocumented medical diagnosis or an incomplete medication list can have serious consequences for the next clinician who picks up the case.
Getting the format for the medical information report right is the first step toward getting the documentation right. The sections below cover a standard general medical report format that works across most clinical settings and specialties.
1. Report header
Start here before anything else. Who prepared this report, what patient does it cover and under what circumstances was it written? Incomplete headers are one of the most common reasons reports get rejected by insurers and delayed in referral pathways. Make sure this section is complete and accurate.
Include:
- Date of report
- Patient’s full name and date of birth
- Patient ID or case number
- Referring physician or requesting organisation
- Treating clinician name, designation and credentials
- Practice or facility name and contact details
2. Reason for report
This is a short paragraph right below the header that explains why a particular medical information report was prepared and who requested it. A report written for an insurance claim is read very differently from one written for a specialist referral. So state the purpose upfront so the receiving party can easily interpret clinical data.
3. Patient information and medical history
This is where most reports create risk. Research suggests that incomplete patient histories are one of the leading contributors to diagnostic errors. When a clinician reads a report, they assume that what is not documented does not exist. A missing allergy is not flagged as unknown, and is read as none. This can result in serious medical issues.
Include:
- Age, gender and occupation
- Chief complaint in the patient’s own words where possible
- History of presenting condition, including onset, duration and severity
- Relevant past medical history, including previous hospitalisations and surgeries
- Current medications with dosages
- Known allergies and previous adverse drug reactions
- Family history where clinically relevant
- Social history, including smoking, alcohol use and living situation
Do not rely on the patient to fill gaps in this section verbally. If information is unavailable, note that explicitly rather than leaving the field blank. A blank field and an unknown field are not the same thing clinically.
Related Read: 15 Medical Poster Examples & Ideas for Patient Education
4. Clinical findings
Keep this section strictly objective. Document what you observed and measured, not what the patient reported. Organize findings by body system and separate them clearly from the history section.
Mixing subjective patient reports with objective clinical data is one of the most cited formatting issues in medical documentation and creates downstream confusion for clinicians acting on the report.
Include:
- Vital signs, including blood pressure, temperature, heart rate and respiratory rate
- General appearance and level of consciousness
- Physical examination findings by body system
- Mental status and functional assessment where relevant
5. Investigations and test results
List every investigation ordered and its result. If results are pending, state that explicitly with the expected date and who is responsible for following up.
Include:
- Laboratory results with reference ranges noted
- Imaging results with radiologist interpretation
- Specialist test results such as ECG, spirometry or biopsy findings
- Date each investigation was conducted
Never leave this section incomplete because you are waiting on results. Write what you have, flag what is outstanding and follow up in writing when results arrive.
6. Assessment and diagnosis
State your assessment directly in this section. If the diagnosis is confirmed, say so. If it is differential, list the possibilities in order of likelihood with the clinical reasoning behind each one. Avoid hedging language without supporting it, like “possible” or “likely.”
Include:
- Primary diagnosis with ICD code where applicable
- Differential diagnoses if the clinical picture is unclear
- Clinical reasoning supporting the assessment
- Diagnoses considered and ruled out with rationale
7. Treatment plan
A receiving clinician or pharmacist should be able to act on this section without needing to contact you for clarification. Vague instructions, such as “continue current medications” or “follow up as needed,” are not a treatment plan. They serve as a gap in the clinical record that the next person in the chain has to fill without your context.
Include:
- Medications prescribed with name, dose, frequency and duration
- Procedures performed or recommended
- Referrals made to specialists or allied health
- Lifestyle and behavioural recommendations
- Patient education provided and whether it was understood and acknowledged
8. Prognosis and follow-up
A report that ends at the treatment plan without clear follow-up instructions is one of the most preventable points of failure in clinical documentation. Be specific about who does what and by when.
Include:
- Expected prognosis in the short and long term
- Follow-up timeframe and who is responsible for arranging it
- Red flag symptoms the patient should monitor
- Conditions under which the patient should seek urgent or emergency care
9. Clinician declaration and signature
This is a legal requirement in most jurisdictions and the accountability anchor for everything in the report above it. Every medical report needs a formal sign-off.
Include:
- Clinician’s full name and designation
- Date of signing
- Signature
- Contact details for clinical queries
Medical report template
Here’s a sample template for medical report you can use.
Medical Report
Date of Report: [Date]
Patient Name: [Full Name]
Date of Birth: [DD/MM/YYYY]
Patient ID / Case Number: [ID]
Treating Clinician: [Name, Designation, Credentials]
Referring Physician / Requesting Organisation: [Name / Organisation]
Facility Contact Details: [Address, Phone, Email]
(State in 2–3 sentences why this report was prepared and who requested it. A referral report and an insurance report are read very differently — stating the purpose upfront frames everything that follows.)
[Write reason for report here…]
(If information is unavailable, note that explicitly. A blank field and an unknown field are not the same thing clinically. Do not leave gaps for the reader to interpret.)
Age / Gender / Occupation: [Write here…]
Chief Complaint (in patient’s own words where possible): [Write here…]
History of Presenting Condition: [Onset, duration, severity, progression — write here…]
Relevant Past Medical History: [Previous hospitalisations, surgeries, chronic conditions — write here…]
Current Medications: [Name / Dose / Frequency — list all…]
Known Allergies and Adverse Drug Reactions: [Write here or state: No known allergies / Unknown]
Family History (where clinically relevant): [Write here or state: Not clinically relevant]
Social History: [Smoking / Alcohol use / Living situation — write here…]
(Objective only. Document what you observed and measured, not what the patient reported. Organise by body system. Do not mix subjective patient reports with objective clinical data in this section.)
| Vital Sign | Reading | Reference Range | Flagged |
| Blood Pressure | [X/X mmHg] | 90/60–120/80 | [Yes / No] |
| Heart Rate | [X bpm] | 60–100 bpm | [Yes / No] |
| Temperature | [X °C] | 36.1–37.2 °C | [Yes / No] |
| Respiratory Rate | [X /min] | 12–20 /min | [Yes / No] |
| Oxygen Saturation | [X]% | 95–100% | [Yes / No] |
General Appearance and Level of Consciousness: [Write here…]
Physical Examination by Body System: [Cardiovascular / Respiratory / Gastrointestinal / Neurological / Musculoskeletal / Other — write findings for each relevant system…]
Mental Status and Functional Assessment (where relevant): [Write here or state: Not assessed / Not clinically indicated]
(List every investigation ordered and its result. If results are pending, state that explicitly with expected date and who is responsible for follow-up. Never leave this section incomplete.)
| Investigation | Date | Result | Reference Range | Flagged |
| [Lab / Imaging / Specialist test] | [Date] | [Result] | [Range] | [Yes / No] |
| [Lab / Imaging / Specialist test] | [Date] | [Result] | [Range] | [Yes / No] |
| [Pending — expected date] | [Date ordered] | Pending | — | Follow-up: [Name] |
Imaging Interpretation: [Radiologist report summary — write here or attach…]
(If the diagnosis is confirmed, say so. If differential, list in order of likelihood with clinical reasoning. Avoid hedging language without supporting it.)
Primary Diagnosis: [Write here] ICD Code: [X]
Differential Diagnoses (if applicable): [List in order of likelihood…]
Clinical Reasoning: [Explain the evidence supporting the assessment…]
Diagnoses Considered and Ruled Out: [Write here with rationale…]
(A receiving clinician should be able to act on this section without contacting you for clarification. Vague instructions are not a treatment plan.)
Medications Prescribed: [Name / Dose / Frequency / Duration — list each…]
Procedures Performed or Recommended: [Write here…]
Referrals Made: [Specialist / Allied health — name, reason, urgency level…]
Lifestyle and Behavioural Recommendations: [Write here…]
Patient Education Provided: [What was explained and whether the patient acknowledged understanding…]
(Be specific about who does what and by when. A report that ends at the treatment plan without clear follow-up instructions is one of the most preventable points of failure in clinical documentation.)
Prognosis (Short-Term): [Write here…]
Prognosis (Long-Term): [Write here…]
Follow-Up Timeframe: [When and with whom…]
Responsible for Arranging Follow-Up: [Clinician / Patient / Practice / Specialist…]
Red Flag Symptoms to Monitor: [Write here — specific symptoms that should prompt the patient to seek review…]
Conditions Requiring Urgent or Emergency Care: [Write here…]
(Legal requirement in most jurisdictions. This is the accountability anchor for everything above it. Every medical report requires a formal sign-off.)
Clinician Full Name: [Name]
Designation and Credentials: [e.g., MBBS, FRACP, Consultant Physician]
Date of Signing: [Date]
Signature: [Wet signature / Digital signature]
Contact for Clinical Queries: [Phone / Email]
Most medical reports are written as continuous text, which makes it difficult for the receiving clinician to quickly locate what they need. In a busy clinical setting, a specialist or insurer should be able to find the diagnosis, medication list and follow-up plan within seconds. That’s why it’s important to visualize healthcare data.
A structured visual template solves this by separating each section into its own clearly labelled block.
- Patient demographics sit in a table at the top.
- Clinical summary has its own dedicated section.
- Discharge details are clearly separated at the bottom.
This makes it easier to process the information correctly.
Venngage medical report template
Venngage’s Medical Report Format Template follows the standard medical report structure covered in this article, with clearly labelled sections for patient demographics, medical and surgical history, clinical summary and discharge details.
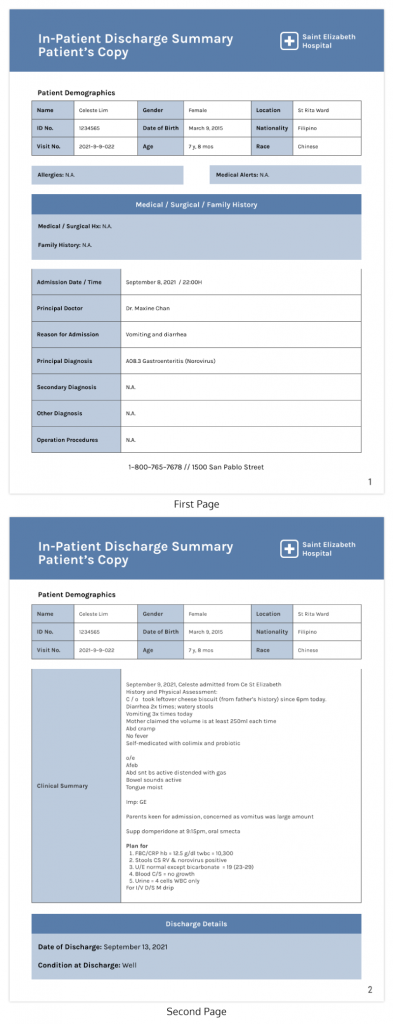
It is well-suited for inpatient settings but can be adapted for outpatient reports and specialist referrals. You can customize it with your facility’s branding, colour scheme and logo using Venngage’s editor and download the final report as a PDF or PNG.
If you want to start from scratch, Venngage’s AI Report Generator lets you describe what you need and builds the layout for you.
Why this medical report format works
A medical report is not just a record of what happened. It is the primary tool through which clinical knowledge passes from one clinician to the next. That’s why a clear format is important. Here’s how it helps:
Mirrors the clinical thinking process
The sections in this format follow the natural sequence of clinical reasoning. History followed by findings, investigations and then eventually diagnosis. This ensures proper treatment. A clinician receiving this report does not have to reconstruct the case.
Makes handoffs safer
Research has shown that communication errors in healthcare, related to handoffs, cause adverse events. A well-structured report is one of the most direct interventions available to reduce that risk. When every section is in a predictable location, the receiving clinician can verify the information easily.
Separates what the patient said from what you observed
Mixing subjective and objective data in a single narrative is one of the most common documentation errors in general practice. This format keeps them in separate sections. The patient history captures what the patient reported. The clinical findings section captures what you observed and measured. That distinction matters when the report is acted on by someone who was not present for the consultation.
Closes the loop on follow-up
The prognosis and follow-up section in this format makes escalation thresholds and next steps explicit. Who arranges the follow-up appointment? What symptoms should prompt urgent review? These are not details the receiving clinician should have to infer.
Pro tips for effective medical report writing
Now let’s some tips to format medical reports better.
Use headers for every section without exception
A report without clear section headers forces the reader to scan the entire document to find what they need. In a clinical setting where decisions are made quickly, that extra time has consequences. Label every section and keep the order consistent across all your reports so that anyone picking one up knows exactly where to look.
Keep each section to its purpose
Clinical findings should contain only what you observed. Patient history should contain only what was reported. The moment you mix the two, the receiving clinician cannot tell what is documented evidence and what is patient recollection. One sentence in the wrong section can change how the report is interpreted.
Use tables for comparative data
Vital signs, investigation results and medication lists are all easier to read in a table than in a paragraph. A well-formatted table lets the reader scan for what is out of range or flagged without reading every value.
Date and time every entry
If a report is updated after the initial consultation, add a dated addendum rather than editing the original text. Overwriting a medical record is a legal and clinical risk. Every addition should be clearly timestamped and attributed.
According to the American Health Information Management Association, precise and reliable information is among the core principles of good clinical documentation.
Flag pending information explicitly
Do not leave blank fields. If a result is outstanding, write “pending — expected [date]” and note who is responsible for follow-up. Incomplete or illegible medical records can result in denied payment and potential recovery of funds already paid.
FAQs on medical report format
1. What should a medical report include?
A comprehensive medical report should cover the report header, reason for report, patient information and medical history, clinical findings, investigations and test results, assessment and diagnosis, treatment plan, prognosis and follow-up, and clinician declaration.
2. What is the difference between subjective and objective findings in a medical report?
Subjective findings are what the patient reports, including symptoms, pain levels and history. Objective findings are what the clinician observes and measures, like vital signs, physical examination results and test data.
3. How long should a medical report be?
There is no fixed length. A general practice report for a referral can be one to two pages. A discharge summary for a complex inpatient case may run longer. What matters is that every section is complete and no information is included without clinical relevance.
4. Who can request a medical report?
Medical reports can be requested by the patient, a specialist receiving a referral, an insurer, a legal team or a government authority. The purpose of the request should be stated in the reason for report section, as it determines how the report should be framed and what level of detail is appropriate.
5. Are medical reports legal documents?
Yes. A medical report is a medicolegal document and can be used as evidence in legal proceedings, insurance claims and regulatory investigations. This is why accuracy, completeness and a signed clinician declaration are non-negotiable in every report, regardless of its primary purpose.